Atrial Fibrillation Treatment & ManagementApproach ConsiderationsThe cornerstones of atrial fibrillation management are rate control and anticoagulation.
[19] The
clinical decision to use a rhythm-control or rate-control strategy
requires an integrated consideration of several factors, including
degree of symptoms, likelihood of successful cardioversion, and presence
of comorbidities. Restoration of sinus rhythm with
regularization of the heart's rhythm improves cardiac hemodynamics and
exercise tolerance. By maintaining the atrial contribution to cardiac
output, symptoms of heart failure and overall quality of life can
improve. As AF contributes to pathologic atrial and ventricular
remodeling, restoration of sinus rhythm can slow or, in some cases,
reverse atrial dilatation and left ventricular dysfunction. For these
reasons, most clinicians focus initially on restoration and maintenance
of sinus rhythm in patients with new-onset AF and opt for a rate-control
strategy only when rhythm control fails. However, several
randomized controlled trials have demonstrated that a strategy aimed at
restoring and maintaining sinus rhythm neither improves survival nor
reduces the risk of stroke in patients with AF. In the AFFIRM
study (Atrial Fibrillation Follow-up Investigation of Rhythm
Management), an insignificant trend toward increased mortality was noted
in the rate control group, and importantly, no evidence suggested that
the rhythm-control strategy protected patients from stroke. In the
study, 4060 subjects aged 65 years or older whose AF was likely to be
recurrent and who were at risk for stroke were randomized to a strategy
of rhythm control (cardioversion to sinus rhythm plus drugs to maintain
sinus rhythm) versus a strategy of rate control (in which no attempt was
made to restore or maintain normal sinus rhythm).
[13] Clinically
silent recurrences of AF in the rhythm-control group are theorized to
be responsible for the increased rates of thromboembolic events and
mortality noted in this cohort. This underscores the importance of
anticoagulation in both rhythm-control and rate-control patients. New
developments aimed at curing AF are being explored actively. By
reducing the critical mass required to sustain AF through either
surgical or catheter-based compartmentalization of the atria (ie, maze
procedure), fibrillatory wavelets collide with fixed anatomic obstacles,
such as suture lines or complete lines of ablation, thus eliminating or
reducing the development of permanent AF. Some patients with focal
origins of their AF also may be candidates for catheter ablation. Still,
much remains to be accomplished before these procedures may be
considered appropriate for primary treatment. Go to Catheter Ablation for complete information on this topic.
Next Section: Risk-Management Decisions
Risk-Management DecisionsOne of the major management decisions in AF (and atrial flutter)
is determining the risk of stroke and appropriate anticoagulation
regimen for low-, intermediate-, and high-risk patients. For each
anticoagulant, the benefit in terms of stroke reduction must be weighed
against the risk of serious bleeding. Overall, approximately
15-25% of all strokes in the United States (75,000/y) can be attributed
to AF. Known risk factors for stroke in patients with AF include male
sex, valvular heart disease (rheumatic valvular disease), heart failure,
hypertension, and diabetes. Additional risk factors, such as advanced
age and prior history of stroke, diabetes, and hypertension, place
patients with preexisting AF at even higher risk for further
comorbidities such as stroke (see Table 1 below).
[20] Table 1. Risk Factors for Stroke in Patients with Nonvalvular Atrial Fibrillation
(Open Table in a new window)| Risk Factors | Relative Risk |
| Prior stroke or TIA | 2.5 |
| History of hypertension | 1.6 |
| Heart failure and/or reduced left ventricular function | 1.4 |
| Advanced age | 1.4 |
| Diabetes | 1.7 |
| Coronary artery disease | 1.5 |
Patients
with rheumatic heart disease and AF have an even higher risk for stroke
(17-fold). At least 4 large clinical trials have clearly demonstrated
that anticoagulation with warfarin decreases the risk of stroke by
50-80%. Most clinicians agree that the risk-benefit ratio of
warfarin therapy in low-risk patients with AF is not advantageous.
Warfarin therapy has, however, been shown to be beneficial in
higher-risk patients with AF. A target international normalized ratio
(INR) of 2-3 is traditionally used in this cohort, as this limits the
risk of hemorrhage while providing protection against thrombus
formation. The appropriate treatment regimen for patients with AF
at intermediate risk is controversial. In this population, the
clinician should assess risk factors for thromboembolic disease, patient
preference, risk of bleeding, risk of falls or trauma, and likelihood
of medication adherence. Warfarin is also superior to clopidogrel or a
combination of clopidogrel and aspirin in the prevention of embolic
events in higher-risk patients. Several risk factor assessment
algorithms have been developed to aid the clinician on decisions on
anticoagulation for patients with AF. The CHADS
2 index (Cardiac failure, Diabetes, Stroke [or S2 = transient ischemic attack]) is the most widely used of these algorithms.
[21] The CHADS
2 index uses a point system to determine yearly thromboembolic risk. Two
points are assigned for a history of stroke or transient ischemic attack
(TIA), and one point is given for age older than 75 years or a history
of hypertension, diabetes, or heart failure. The predictive value of
this scoring system was evaluated in 1733 elderly patients with
nonvalvular AF aged 65-95 years who were not given warfarin at hospital
discharge. Although high scores were associated with an increased rate
of stroke, few patients had a score greater than 5 or a score of 0 (see
Table 2 below). However, the
CHA2DS2-VASc(CHA2DS2-Vasculardisease,Age65-74years,Sexcategory)scorebetterpredictspatientsathigh-riskaswellasthosecategorized
at low risk for thromboembolism.
[22] Table 2. Adjusted Stroke Rate in Patients with Nonvalvular Atrial Fibrillation not Treated with Anticoagulation
(Open Table in a new window)| CHADS2 Score | Adjusted Stroke Rate (%/y) |
| 0 | 1.9 |
| 1 | 2.8 |
| 2 | 4.0 |
| 3 | 5.9 |
| 4 | 8.5 |
| 5 | 12.5 |
| 6 | 18.2 |
Recommendations
on anticoagulation for patients with nonvalvular AF are based on the
2006 American College of Cardiology (ACC)/American Heart Association
(AHA)/European Society of Cardiology (ESC) task force guidelines on the
management of patients with atrial fibrillation (see Table 3 below).
[20] Table 3. Recommendations for Antithrombotic Therapy in Patients with Nonvalvular Atrial Fibrillation
(Open Table in a new window)| Risk Category | Recommended Therapy |
| No risk factors | Aspirin 81-325 mg daily |
| One moderate-risk factor | Aspirin 81-325 mg daily or warfarin (INR 2-3) |
| Any high-risk factor or more than 1 moderate-risk factor | Warfarin (INR 2-3) |
High-risk
factors include prior stroke, TIA, and systemic thromboembolism.
Moderate-risk factors include age older than 75 years, hypertension,
heart failure, left ventricular function less than 35%, and diabetes
mellitus. Risk factors of unknown significance include female sex, age
65-74 years, coronary artery disease, and thyrotoxicosis.
Previous
Next Section: Risk-Management Decisions
Management of New-Onset AFThe AFFIRM study and similar findings from the smaller Rate Control Versus Electrical Cardioversion (RACE) trial
[23] have
led to the development of consensus guidelines that recommend an
initial rate-control strategy for many asymptomatic patients with atrial
fibrillation. The ACC/AHA/ESC 2006 guidelines state that an
initial rate-control strategy is "reasonable" for asymptomatic or
minimally symptomatic older patients with hypertension and comorbid
cardiovascular disease.
[20] These
same guidelines state that for younger individuals, especially those
without significant comorbid cardiovascular disease, an initial
rhythm-control strategy may be a better approach.
Rate controlRegardless
of the long-term management strategy chosen, control of ventricular
rate is a critical component of management of new-onset AF. The main
determinants of the ventricular rate during AF are those intrinsic and
extrinsic factors that influence atrioventricular (AV) conduction.
Foremost among these are the intrinsic AV nodal conduction properties.
Underlying sympathetic and parasympathetic tone also influences AV nodal
conduction. Rate-controlling agents act primarily by increasing AV
nodal refractoriness. Beta-blockers and calcium channel blockers
are first-line agents for rate control in AF. These drugs can be
administered either intravenously or orally. They are effective at rest
and with exertion. Intravenous diltiazem or metoprolol are commonly used
for AF with a rapid ventricular response. Caution should be exercised
in patients with reactive airway disease who are given beta-blockers. Digoxin
can be used in the acute setting but does little to control the
ventricular rate in active patients. As such, it is rarely used as
monotherapy. Caution should be exercised in elderly patients and those
with renal failure receiving digoxin. Digoxin is indicated in patients
with heart failure and reduced LV function. Amiodarone has a
class IIa recommendation from the ACC/AHA/ESC for use as a
rate-controlling agent for patients who are intolerant of or
unresponsive to other agents, such as patients with CHF who may
otherwise not tolerate diltiazem or metoprolol. Caution should be
exercised in those who are not receiving anticoagulation, as amiodarone
can promote cardioversion. Extreme care must be taken in patients
with preexcitation syndrome and AF. Blocking the AV node in some of
these patients may lead to AF impulses that are transmitted exclusively
down the accessory pathway, and this can result in ventricular
fibrillation. (If this happens, the patient will require immediate
defibrillation.) Calcium channel blockers and digoxin are
contraindicated in these patients; flecainide or amiodarone can be used
instead.
[24] AnticoagulationOne
of the most important considerations in the acute management of atrial
fibrillation is the need for anticoagulation (see the image below).
Acute cardioversion for AF carries a risk of thromboembolism unless
anticoagulation therapy is initiated prior to the procedure and
continued post procedure. Risk of thromboembolism is similar in patients
undergoing either pharmacologic or electrical cardioversion. The risk
of thromboembolic events is greatest when AF has been present for longer
than 48 hours. Effective anticoagulation in patients with AF reduces
the risk of stroke 3-fold.

Patient
management for newly diagnosed atrial fibrillation. Subtherapeutic INR:
INR < 2 for 3 consecutive weeks. Warfarin: INR target 2-3.
TEE/cardioversion: low molecular weight heparin 1 mg/kg bid as a bridge
with initiation of warfarin INR 2-3. Patients
with newly diagnosed AF and patients awaiting electrical cardioversion
can be started on intravenous heparin (activated partial thromboplastin
time [aPTT] of 45-60 seconds) or low-molecular-weight heparin (1 mg/kg
bid). Patients can be started concomitantly on warfarin in an
inpatient setting while awaiting a therapeutic INR value (2-3). Many
practices have developed specialized anticoagulation clinics to monitor
INR values closely. Oral direct thrombin inhibitors may present an
alternative to warfarin in a higher-risk population with nonvalvular AF.
In the highest-risk population (eg, AF with valvular heart
disease or prior embolic cerebrovascular accident), bridging
anticoagulation with heparins may be required in the periprocedural
period.
CardioversionCardioversion may be performed
electively or emergently to restore sinus rhythm in patients with
new-onset atrial fibrillation. Cardioversion is most successful when
initiated within 7 days after onset of AF. The need for cardioversion
may be acute when AF is responsible for hypotension, heart failure, or
angina. Pharmacologic agents or direct current energy can be used
to cardiovert patients with AF. Pharmacologic cardioversion has the
advantage of not requiring sedation or anesthesia, but the major
disadvantage is the risk of ventricular tachycardia and other serious
arrhythmias.
Previous
Next Section: Risk-Management Decisions
Long-Term ManagementLong-term
management of atrial fibrillation is focused on reducing the likelihood
of AF recurrence, reducing AF-related symptoms, control of ventricular
rate, and reducing stroke risk. As discussed previously, AF is often the
result of established cardiovascular risk factors. Appropriate
management of these risk factors will reduce the likelihood of future
episodes of AF and AF-related morbidity and mortality. Anticoagulation
with either aspirin or warfarin should be initiated for all individuals
with AF, except those with lone AF or contraindications. Selection of
the appropriate antithrombotic regimen for a given patient should be
balanced between the risk of stroke and the risk of bleeding.
Antiarrhythmic therapy can aid in maintenance of sinus rhythm in certain
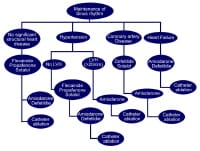
patients but requires close monitoring. Optimal long-term
strategies for AF management should be based on a thoroughly integrated
consideration of patient-specific factors and likelihood of success. As a
rule, younger patients with more severe symptoms and fewer
comorbidities tend to derive greater benefit from a long-term focus on
rhythm control. Older patients with structural heart disease (eg, left
ventricular hypertrophy, prior MI, depressed ejection fraction, atrial
dilation) are less likely to remain in sinus rhythm and are more likely
to have serious side effects from antiarrhythmic drugs. In this cohort,
most clinicians focus on long-term rate control. Because of the
electrophysiologic and structural remodeling caused by AF, many patients
with paroxysmal AF will progress to persistent and permanent AF. The
degree to which this reflects the continuing influence of underlying
cardiovascular risk factors as opposed to a direct effect of AF is
unknown. Regardless, clinicians need to reevaluate their management
strategies frequently, as AF burden and comorbidities increase with
time.
AnticoagulationThe goal of long-term
anticoagulation in atrial fibrillation is to reduce the risk of
thromboembolism. Patients in AF have a risk of stroke or peripheral
embolism that is approximately 5 times that of individuals in sinus
rhythm. Recommendations for anticoagulation for patients with
nonvalvular AF are based on guidelines from a 2006 ACC/AHA/ESC task
force on the management of patients with atrial fibrillation.
[2] Anticoagulation
therapy with warfarin is significantly more effective than antiplatelet
therapy (relative risk of 40%) if the INR is adjusted. The INR goal in
AF is usually between 2 and 3, except in patients who are at a
significant risk for stroke (eg, patients with artificial valves, those
with rheumatic heart disease, and those at a high risk for AF with
recurrent prior strokes), in whom the INR should be maintained between
2.5 and 3.5. A lower INR goal (1.8-2) may be considered in elderly
patients who are at high risk for a fall. Anticoagulation clinics
have shown more success and a lower complication rate than primary care
physicians in controlling patients’ INR. In addition, one study
reported that patients who used an Internet-based program for patient
self-management of oral anticoagulant therapy achieved a higher mean
time in the therapeutic range than patients whose INR was controlled by
an established anticoagulation clinic.
[25] Similar
programs alone or in combination with regular care provided by
anticoagulation clinics may improve the mean time that patients are in
the therapeutic range and may further reduce the risk of stroke. As
patients with AF age, the relative efficacy of oral anticoagulation
appears not to decrease, whereas the efficacy of antiplatelet therapy
does appear to decrease, according to a study by van Walraven.
[26] The
major adverse effect of anticoagulation therapy with warfarin is
bleeding. Factors that increase this risk include the following:
- History of bleeding (the strongest predictive risk factor)
- Age older than 75 years
- Liver or renal disease
- Malignancy
- Thrombocytopenia or aspirin use
- Hypertension
- Diabetes mellitus
- Anemia
- Prior stroke
- Fall risk
- Genetic predisposition
- Supratherapeutic INR
Several risk models have been introduced. The risk model called HEMORR2HAGES assigns points to risk factors, as follows
[27] :
- History of bleeding (2 points)
- Hepatic or renal disease (1 point)
- Alcohol abuse (1 point)
- Malignancy (1 point)
- Older age (>75 y) (1 point)
- Reduced platelet count or function, including aspirin therapy (1 point)
- Hypertension (1 point)
- Anemia (1 point)
- Genetic predisposition (1 point)
- Excessive fall risk (1 point)
- Stroke (1 point)
Using this scoring, the risks of a major bleeding event per 100 patient-years of warfarin therapy are as follows:
- 0 points - 1.9%
- 1 point - 2.5%
- 2 points - 5.3%
- 3 points - 8.4%
- 4 points - 10.4%
- 5 or more points - 12.3%
When
the bleeding risk outweighs the benefit, avoidance of anticoagulation
therapy in AF should be considered. In addition, because of its
teratogenic effects, anticoagulation with warfarin is contraindicated in
pregnant women, especially in the first trimester. According to
the 2011 update to ACCF/AHA/HRS guidelines on atrial fibrillation, if
warfarin will not be used, adding clopidogrel to aspirin may be
considered.
[28] The
RE-LY study evaluated the efficacy and safety of 2 different doses of
dabigatran relative to warfarin in more than 18,000 patients with atrial
fibrillation. Patients were randomized to 1 of 3 arms: (1) adjusted
dose warfarin, (2) dabigatran 110 mg bid, or (3) dabigatran 150 mg bid.
Dabigatran 110 mg was noninferior to warfarin for the primary efficacy
endpoint of stroke or systemic embolization, while dabigatran 150 mg was
significantly more effective than warfarin or dabigatran 110 mg. Major
bleeding occurred significantly less often with dabigatran 110 mg than
warfarin; dabigatran 150 mg had similar bleeding to warfarin.
[29, 30] Guidelines
from the American College of Cardiology Foundation (ACCF)/American
Heart Association (AHA)/Heart Rhythm Society (HRS) on atrial
fibrillation have been updated to include the use of oral direct
thrombin inhibitors (ie, dabigatran).
[31] The
guidelines include a class Ib recommendation (ie, treatment is
useful/effective based on a single randomized trial) for dabigatran. The
guidelines recommend dabigatran may be used as an alternative to
warfarin for the prevention of stroke and systemic thromboembolism in
patients with paroxysmal-to-permanent atrial fibrillation and risk
factors for stroke or systemic embolization. Patients with atrial
fibrillation who are not candidates include those with prosthetic heart
valves or hemodynamically significant valve disease, severe renal
failure (creatinine clearance ≤15 mL/min), or advanced liver disease.Anticoagulation
prior to and during an elective surgery may be continued or stopped
depending on the patient’s risk of bleeding and risk of thromboembolism.
If the risk of thromboembolism is high (stratified by the CHADS
2 score) and the risk of bleeding is low, anticoagulation should be
continued with the INR in the low therapeutic range. However, a high
risk of bleeding during the procedure should prompt discontinuation of
warfarin for 3-5 days prior to surgery. These patients should then be
treated with heparin prior to and following the operation to allow
discontinuation of anticoagulation if bleeding occurs. In
general, patients who develop AF only postoperatively do not need
anticoagulation. Administration of preoperative and postoperative
beta-blockers is usually sufficient, as postoperative AF is usually
paroxysmal and tends to terminate spontaneously. A mutation in
coagulation factor IX may cause spontaneous bleeding even with INR in
the therapeutic range. Adverse effects of warfarin therapy are not
limited to bleeding, however; other important side effects include skin
necrosis within the first few days of therapy and cholesterol
embolization to the skin or visceral organs in the first few weeks of
therapy.A large cohort study in Denmark compared bleeding risk of
anticoagulants prescribed upon hospital discharge for atrial
fibrillation. During mean follow-up (3.3 y), 11.4% of patients
experienced a nonfatal or fatal bleeding episode. The highest incidence
for bleeding was observed for dual therapy with warfarin and clopidogrel
and for triple therapy with warfarin, aspirin, and clopidogrel (3-fold
higher risk) compared with single agent use.
[32] Omega-3 fatty acidsSeveral
small trials have suggested that treatment for paroxysmal AF with
prescription omega-3 fatty acids may provide a safe and effective
treatment option. However, no benefit has been found to date.
[33] Angiotensin converting enzyme (ACE) inhibitors and ACE receptor blockers (ARB)Trials
examining the incidence of AF in patients with heart failure who are
treated with ACE inhibitors or ARBs have demonstrated a potential
beneficial effect on AF recurrence. This recurrence is thought to be
mediated by blocking the rennin-angiotensin-aldosterone system and the
downstream effects on atrial mechanical and electrical remodeling.
[34, 35, 36] A
study by Yusuf et al examined the effects of irbesartan in patients
with permanent AF or at least 2 episodes of paroxysmal AF in the
previous 6 months.
[37] Irbesartan
did not demonstrate a benefit in patients with AF who were already
receiving an ACE inhibitor or patients in sinus rhythm. No reduction in
cardiovascular death, stroke, or myocardial infarction was noted in the
patient population studied.
Rate controlAs discussed
previously, several trials have validated the noninferiority of an
initial rate-control strategy. Many clinicians believe, however, that an
attempt at a rhythm-control strategy should be made in most patients.
Older patients with comorbid cardiovascular disease have a lower
likelihood of successful long-term rhythm control, and thus, these
patients are often managed using a rate-control strategy. Some patients
managed initially with a rhythm-control strategy will progress to
recurrent or persistent AF. Clinicians often switch to a rate-control
strategy as the AF burden increases. Effectiveness of rate
control should be assessed both at rest and with exertion, especially in
patients who experience primarily exertional AF-related symptoms.
Twenty-four hour Holter monitoring or exercise-treadmill testing can be
helpful in evaluating heart rate variability. Adequate rate
control was previously defined as a heart rate of 60-80 bpm at rest and
90-115 bpm with moderate exercise. However, ACCF/AHA/HRS guidelines on
management of atrial fibrillation were updated in 2011 to state that
there was no benefit in achieving strict heart rate control (< 80 bpm
at rest, < 110 bpm after a 6-minute walk) relative to more lenient
rate control (< 110 bpm at rest). Strict rate control in patients
with stable ventricular function is no longer recommended.
[28] AV
nodal blocking medications are the cornerstone of rate control in
long-standing AF. In the absence of an accessory pathway, oral
beta-blockers, nondihydropyridine calcium channel blockers, and digoxin
are effective. Generally, coadministration of beta-blockers and calcium
channel blockers is reserved for patients in whom adequate rate control
cannot be achieved with a single agent. Digoxin can be effective
in sedentary patients (especially in those with heart failure) but
requires close monitoring of drug levels and renal function.
Combinations of rate-control medications (eg, beta-blocker and digoxin)
may be superior to individual agents in some patients. Amiodarone
may contribute to ventricular rate control. On the other hand,
antiarrhythmic agents may organize AF to a potentially life-threatening
atrial flutter with 1:1 AV conduction. Particularly with class IC
agents, maintenance of effective AV nodal rate control is essential in
most patients. Therefore, administration of a beta-blocker or calcium
channel blocker is recommended before class IC drugs are initiated. In
the presence of tachycardia-mediated cardiomyopathy or inadequate
ventricular rate control despite drug therapy, AV nodal ablation and
pacemaker implantation may be considered.
Rhythm controlMaintenance
of sinus rhythm requires treatment of cardiovascular risk factors and
any underlying disorder (ie, hyperthyroidism) that may have triggered
AF. As mentioned previously, several antiarrhythmic drugs (flecainide,
propafenone, dofetilide, amiodarone) have established efficacy in the
pharmacologic conversion of AF to sinus rhythm. The noncardiac adverse
effects and contraindications of each drug should be checked prior to
administration. Amiodarone, as a part of a strategy to achieve
sinus rhythm, appears to be safe and effective in patients with
persistent AF, according to Doyle and Ho. However, in their study,
intolerable adverse effects were more common with amiodarone than with
placebo or rate-control drugs.
[38] Nevertheless,
in patients with cardiac disease such as coronary artery disease or
systolic or diastolic heart failure, amiodarone becomes the drug of
choice because of its decreased proarrhythmic effects compared with
other antiarrhythmic drugs.
[24] Amiodarone
was also found to be more effective at maintaining sinus rhythm than
other drugs in the Canadian Trial of Atrial Fibrillation (CTAF) and the
Sotalol Amiodarone Atrial Fibrillation Efficacy Trial (SAFE-T).
[39, 40] The
2011 update to the ACCF/AHA/HRS AF guideline adds that it is reasonable
to use dronedarone to reduce the probability that hospitalization will
be required for patients with paroxysmal AF or after conversion of
persistent AF. Class IV heart failure or a recent episode of
decompensated heart failure are contraindications.
[28] Several
distinct agents, most notably sotalol, are used for the long-term
maintenance of sinus rhythm. Sotalol is efficacious, but as with other
class III drugs, it requires close monitoring of the QT interval and
serum electrolytes. Sotalol is associated with the risk of QT interval
prolongation and torsade de pointes.
The proarrhythmic effect of sotalol is increased in patients with CHF
(unlike dofetilide and amiodarone), so it is generally contraindicated
in such patients or in those with a prolonged QT interval. Hypokalemia
should be corrected and monitored prior to administration of sotalol
because it may also prolong the QT interval. Sotalol can be used in
patients with coronary artery disease.
[24] Class
III agents (sotalol, amiodarone) also have some beta-blocking effect
and should be used with caution in patients with a history of
bradycardia. Class Ic drugs increased the mortality risk in
patients with coronary artery disease during the Cardiac Arrhythmia
Suppression Trial (CAST) and therefore should not be used in these
patients.
[41] Class
Ic drugs increased the mortality risk in patients with coronary artery
disease during the Cardiac Arrhythmia Suppression Trial (CAST) and
therefore should not be used in these patients.
[39] Catheter
ablation performed in experienced centers is recommended in the 2011
update to the ACCF/AHA/HRS AF guidelines for several indications:{Ref55}
- It is recommended as an alternative
to pharmacologic therapy to prevent recurrent paroxysmal AF in
significantly symptomatic patients with little or no structural heart
disease[40] or severe pulmonary disease (Class I, evidence level A).
- It is reasonable as a treatment for symptomatic persistent AF.
- Catheter ablation may be reasonable as a treatment for symptomatic paroxysmal AF in patients with some structural heart disease.
Surgical
ablation of AF is also an option for patients with AF undergoing other
cardiac surgery and for those patients in whom pharmacologic and
catheter-based procedures are ineffective or contraindicated. Atrial
fibrillation ablation may be superior to AV nodal ablation and
biventricular pacing in heart failure patients but is technically
difficult and demanding, and the widespread applicability of ablation in
this population of patients is uncertain. Go to Catheter Ablation for complete information on this topic.New
medical and device-based rhythm-control therapies are being explored
actively. Experimental and clinical data suggest that renin-angiotensin
system (RAS) antagonists and HMG-CoA-reductase inhibitors (statins) may
decrease the incidence of AF and increase the likelihood of successful
cardioversion.
[42, 43, 44, 45] Device-based therapies under investigation include single- and dual-site atrial pacemakers
to prevent AF, as well as atrial defibrillators to rapidly restore
sinus rhythm. Invasive (surgical and catheter-based) therapies to
compartmentalize the atria and localize focal triggers (in the pulmonary
veins) are being evaluated and refined. (See Surgical Care.)
Electrical cardioversionPatients
who are hemodynamically unstable, who have severe dyspnea or chest pain
with atrial fibrillation, or who have preexcited atrial fibrillation
should undergo urgent cardioversion.
[24] In
stable patients with symptomatic new-onset AF, the rate-control
strategy may be considered first to control the ventricular rate. If
rate-control treatment does not elicit a response or if echocardiography
does not reveal any valvular or functional abnormality of the heart,
cardioversion is indicated. DC cardioversion is the delivery of
electrical current that is synchronized to the QRS complexes; it can be
delivered in monophasic or biphasic waveforms. The required energy for
cardioversion is usually 100-200 J (sometimes higher energy is required)
for monophasic waveforms and less for biphasic waveforms. The patient
should be sedated. In patients with AF of relatively short duration in
whom the left atrium is not significantly large, the success rate of
cardioversion exceeds 75% (ie, the size of the left atrium and the
duration of AF inversely correlate with the success rate of
cardioversion). Embolization is the most important complication
of cardioversion. Accordingly, thrombus in the heart should be ruled out
with transesophageal echocardiography, or warfarin should be given for
anticoagulation for 4 weeks before cardioversion is performed. Stunning
of the atria and stasis can occur after cardioversion, and this can lead
to thrombus formation even though the patient is in sinus rhythm.
Therefore, the patient should receive anticoagulants for at least 4
weeks following the procedure. Other complications of electrical
cardioversion may include pulmonary edema, hypotension, myocardial
dysfunction, and skin burns, which may be avoided with the use of
steroid cream and proper technique. Electrical cardioversion is also
associated with some ST- and T-wave changes on ECG and may elevate
levels of serum cardiac biomarkers. Synchronization prevents serious
ventricular arrhythmias. Placement of pads or paddle positions
include anterior-lateral (ventricular apex and right infraclavicular)
and anterior-posterior (sternum and left scapular), with at least one
study suggesting increased efficacy with the anterior-posterior (AP)
method. Biphasic waveforms are proved to convert AF at lower
energies and higher rates than monophasic waveforms. Strategies include
dose escalation (70, 120, 150, 170J for biphasic or 100, 200, 300, 360J
for monophasic) versus beginning with single high energy/highest success
rate for single shock delivered. Patients who are stable and/or awake
and can tolerate sedation should be pretreated, with typical regimens
involving midazolam, fentanyl, and propofol. Cardioversion of
patients with implanted pacemakers and defibrillator devices is safe
when appropriate precautions are taken. Keeping the cardioversion pads
in an AP orientation ensures that the shocks are not directly over the
generator. Alteration in pacer-programmed data has been reported, as
well as heart block and elevated enzymes if the current is conducted
through a pacer lead.
Pharmacologic cardioversionAlthough
pharmacologic cardioversion may be used as the first-line strategy, it
is used mainly if DC cardioversion fails or, in some cases, as a
precardioversion strategy. Out-of-hospital self-administration of
either flecainide 300 mg or propafenone 600 mg (weight-based dosages if
>70 kg) was determined to be successful in terminating AF in 94% of
episodes (mean time to symptom resolution of 133 minutes) by Alboni et
al. The investigators studied outpatient treatment of atrial
fibrillation with a “pill-in-the-pocket” approach in 268 patients with
little or no structural heart disease presenting to the emergency
department with symptomatic AF.
[46] Pretreatment
with amiodarone, flecainide, ibutilide, propafenone, or sotalol has
been shown to increase the success rate of DC cardioversion and is
recommended by the American College of Cardiology.
[2] This strategy is also recommended when DC cardioversion fails and prior to repeat DC cardioversion.
[2] Intravenous
amiodarone is typically given as a 150-mg bolus over 10-15 minutes,
followed by a continuous infusion of 1 mg/min for 6 hours and then 0.5
mg/min. Hemodynamically unstable patients (eg, those with
hypotension) may not tolerate antiarrhythmic drugs, and the adverse
effects and contraindications of each antiarrhythmic drug should be
considered carefully before administration. Because of possible
proarrhythmic adverse effects of antiarrhythmic drugs, these patients
should be monitored for at least 24 hours, requiring hospitalization in
most cases. The ACC/AHA/ESC guidelines provide the following recommendations regarding pharmacologic conversion of atrial fibrillation
[47] :
- For
conversion of AF of 7 days or less, agents with proven efficacy include
dofetilide, flecainide, ibutilide, propafenone, and, to a lesser
degree, amiodarone and quinidine; less effective or incompletely studied
agents include procainamide, digoxin, and sotalol.
- For
conversion of AF lasting 7-90 days, agents with proven efficacy include
dofetilide, amiodarone, ibutilide, flecainide, propafenone, and
quinidine; less effective or incompletely studied agents include
procainamide, sotalol, and digoxin.
- For
conversion of AF lasting more than 90 days, oral propafenone,
amiodarone, and dofetilide have been shown to be effective at converting
persistent AF to normal sinus rhythm (NSR).
The US
Food and Drug Administration (FDA) mandates inpatient monitoring for
dofetilide initiation. Patients who start sotalol usually require
inpatient monitoring (for torsade de pointes), although patients with no
heart disease, with a QT interval less than 450 msec, and with normal
electrolytes should be started on outpatient medications.In 2010,
the American Heart Association-American Stroke Association (AHA-ASA)
issued its guidelines for the primary prevention of stroke, which
included the note that screening patients over 65 years of age for AF in
the primary care settings using pulse taking followed by an ECG may be
useful. Adjusted-dose warfarin should be used for all patients with
nonvalvular AF (target INR 2-3). Aspirin is recommended for low and
moderate-risk patients with AF and for high-risk patients unsuitable for
anticoagulation; a combination of clopidogrel and aspirin may
protection against stroke than aspirin alone.
[48] Special considerationsPostoperative
AF is common, and perioperative beta blockers are recommended in all
patients undergoing cardiac surgery unless contraindicated.
[49] Preoperative
administration of amiodarone and sotalol may reduce the incidence of AF
in patients undergoing cardiac surgery. As such, these agents may be
used as prophylactic therapy in those at high risk for postoperative AF.
Retrospective data suggest that atrial-based pacing (AAI, DDD
modes) reduces the risk of developing AF and increases the interval
between episodes in patients with sick sinus syndrome.
[50] Previous
Next Section: Risk-Management Decisions
Overview of Surgical and Catheter Ablation The
goal of catheter ablation and surgical treatment of atrial fibrillation
is to disconnect triggers and/or to modify the substrate for AF.
Mapping and radiofrequency (RF) ablation of AF is one of the most
complex ablation procedures. Numerous approaches are used depending on
the expertise of the cardiac electrophysiologist and characteristics of
the AF. Paroxysmal AF is usually caused by triggered and ectopic
activity in pulmonary veins, and ablation around the veins terminates
the arrhythmia. In persistent AF, triggering foci and reentry circuits
may coexist in the atrial tissue, requiring more extensive mapping and
ablation to terminate the AF; this yields a lower success rate than
ablation used to treat paroxysmal AF.Aniarrhythimic drug (AAD)
treatment for 6 weeks after ablation of paroxysmal AF was shown to be
well tolerated, to reduce the incidence of clinically significant atrial
arrhythmias, and to reduce the need for cardioversion or hospital
admission during that period, according to Roux et al. Class IC drugs
were used as the first line of therapy, and sotalol was the most
commonly used drug in cases of LV dysfunction or CAD. Measured outcomes
included atrial arrhythmias lasting more than 24 hours; atrial
arrhythmias associated with severe symptoms that required
hospitalization, cardioversion, or initiation/change of antiarrhythmic
drug therapy; and intolerance to antiarrhythmic agent requiring drug
cessation.
[51] Previous
Next Section: Risk-Management Decisions
Compartmentalization of the AtriaTwo
approaches to compartmentalization of the atria are surgical, by which
multiple cuts are made to the atria, and radiofrequency ablation.
Surgical compartmentalization of the atria (maze procedure)Since
its inception, surgical compartmentalization of the atria, or the
“maze” procedure, has evolved as an exciting approach with the potential
to cure atrial fibrillation. The procedure involves making a series of
small endocardial incisions in the right and left atria to isolate the
pulmonary veins and interrupt potential reentrant pathways required for
AF maintenance. Early experience showed that atrial transport is
restored postoperatively and that long-term anticoagulation is not
required. The downside remains the need for an open chest
procedure; however, thoracoscopic procedures may reduce hospitalization
and recovery times in the future. The maze procedure remains an
attractive procedure for patients with AF who are undergoing concomitant
mitral valve procedures. Its role as a primary therapy for AF is
doubtful. The role of lesion sets on outcome after maze procedure was
studied; the addition of right-sided ablation was found to improve
clinical and electrophysiologic results after maze procedure.
[52] Compartmentalization of the atria with continuous ablation lines of blockageAs
a parallel to the maze procedure, electrophysiologists are attempting
to mimic surgical suture lines with radiofrequency lesions. The
procedures tend to last many hours, and success rates are somewhat
disappointing (50-60%), with the occurrence of left atrial reentrant
tachycardias and left atrial flutters (requiring further ablation
procedures).
[53] Researchers
are unsure which areas of the atria are necessary to sustain AF. Purely
right-sided lesions are not sufficient to eliminate AF, making left
atrial procedures necessary. In addition, gaps in linear lesions can be
difficult to find. Research currently focuses on catheter design
to deliver linear continuous lesions. Additionally, alternative energy
sources (eg, cryotherapy, laser, ultrasound) may improve the ability to
deliver transmural lesions in the left atrium.
Previous
Next Section: Risk-Management Decisions
Catheter Ablation of Focal Triggers of AF In some patients, AF appears to be triggered by electrically active pulmonary vein foci.
[54] These
patients typically have an abundance of ectopic atrial beats noted on
24-hour Holter monitoring. Electrical isolation of individual pulmonary
veins, and thus the ectopic foci, is performed successfully at many
centers, and patient selection is key to success. A combined
procedure including individual pulmonary vein isolation, as well as left
atrial ablation (ie, encircling pulmonary vein pairs, connecting right
and left pairs along the left atrial roof, and connection to the mitral
valve annulus), is often necessary. Chest CT or MRI can be used to
recreate 3-dimensional anatomy in the left atrium, thus aiding in
mapping and creating contiguous lines in the left atrium, as displayed
in the video below.The
image on the right is a reconstructed 3-dimensional image of the left
atrium in a patient undergoing atrial fibrillation ablation. The figure
on the left was created with a mapping catheter using Endocardial
Solutions mapping technology. It represents the endocardial shell of the
left atrium and is used as the template during left atrial ablation
procedures. Patients with paroxysmal AF
in whom antiarrhythmic drug therapy does not elicit a response are
potential candidates for RF ablation of AF. The threshold for catheter
ablation has fallen over the years and is likely to continue to fall.
Ablation of persistent AF is more complex and yields lower success
rates. Therefore, RF ablation is an option only if antiarrhythmic drugs
fail in patients with persistent AF who remain severely symptomatic
despite adequate ventricular rate control.
[55] The
success rate of RF ablation in the treatment of AF varies depending on
the type and duration of AF (ie, paroxysmal vs persistent), structural
remodeling of the heart, and the technique and expertise of the cardiac
electrophysiologist, but it usually ranges from 60-80% over 1-2 years of
follow-up. Complications associated with RF ablation of AF
include cardiac perforation, pericardial effusion, cardiac tamponade,
vascular access complications, pulmonary vein stenosis, thromboembolism,
atrioesophageal fistula, and left atrial flutter. Pulmonary vein
stenosis develops in about 6% of patients and may cause dyspnea, chest
pain, cough, and hemoptysis.
[2] If
pulmonary vein stenosis is suspected following RF ablation, further
diagnostic workup with TEE, spiral CT scanning, or MRI is recommended.
MRI is the most accurate test in diagnosing this complication. Patients
with pulmonary vein stenosis should undergo percutaneous angioplasty,
which can significantly improve pulmonary blood flow and the patient's
symptoms. Go to Catheter Ablation for complete information on this topic.
Previous
Next Section: Risk-Management Decisions
AV Node Ablation and Permanent Pacemakers AV
node ablation may be an alternative in patients with persistent AF and
an uncontrolled ventricular response despite aggressive medical therapy.
Catheter ablation of the AV junction permanently interrupts conduction
from the atria to the ventricles. Because the result is permanent
AV block, a permanent ventricular pacemaker is required. AF may still
be present, but the pacemaker governs the ventricular response. The risk
of thromboembolism is unchanged, and patients still require
anticoagulation; however, most patients are relieved of their symptoms.
During the first 1-3 months, the pacing rate must be programmed in the
80- to 90-beat range to prevent torsade de pointes, which presumably
occurs because of slow ventricular rates and early
after-depolarizations. In patients with significant ventricular
dysfunction and permanent ventricular pacing, a biventricular device may
be appropriate.
[56] Improvements in LV size and function, functional class, and quality-of-life scores have been demonstrated.
[57] Previous
Next Section: Risk-Management Decisions
Left Atrial Appendage Percutaneous Closure Embolic
stroke in patients with nonvalvular AF is thought to be associated with
left atrial appendage (LAA) thrombi. LAA closure may be a suitable
alternative to chronic warfarin therapy for stroke prophylaxis in
patients with nonvalvular AF, according to Holmes and colleagues. The
investigators compared the efficacy and safety of LAA percutaneous
closure with warfarin therapy in patients with AF, and follow-up at the
point of 1065 patient-years showed the intervention group (LAA closure
without warfarin treatment) event rate was 3 per 100 patient-years
compared with the control group (patients given warfarin) event rate of
4.9 per 100 patient-years.
[58] Previous
Next Section: Risk-Management Decisions
Consultations Consultation
with a cardiac electrophysiologist or knowledgeable clinician is
recommended prior to antiarrhythmic drug initiation.A
cardiologist may be consulted emergently if complicating factors are
present or if the patient is experiencing ongoing cardiac ischemia or
infarction not treatable with DC cardioversion, rate-reduction measures,
and standard chest pain protocols.
[59] A
patient with acute myocardial infarction (AMI) and new-onset AF who is
stable may benefit from simple rate-control measures (eg, intravenous
beta-blockers) while being prepared for the catheterization laboratory
and while intravenous nitrates, heparin, and aspirin are begun. In the
patient with an ST elevation MI, the main emphasis, however, is to
minimize door-to-open-artery time. A patient's cardiologist plays
a vital role in determining the most appropriate long-term strategy for
a patient with AF and provides crucial follow-up care.
Previous
Next Section: Risk-Management Decisions
Long Term MonitoringRF ablation of atrial fibrillationPatients
who undergo RF ablation of atrial fibrillation should be monitored for
the signs and symptoms of potential complications, such as the
following:
- Cardiac perforation
- Pericardial effusion
- Cardiac tamponade
- Vascular access complications
- Pulmonary vein stenosis
- Thromboembolism
- Atrioesophageal fistula
- Left atrial flutter
In
addition, AF can recur and most episodes are asymptomatic. Therefore,
it is important to monitor for signs and symptoms of recurrent AF in
follow-up visits and to administer appropriate diagnostic tests if
recurrence is suspected.
Further outpatient careAssessment
and reassessment of thromboembolic risk is necessary, and periodic ECG
monitoring (especially when taking antiarrhythmics) and Holter
monitoring are often necessary to assess for paroxysmal AF and/or rate
control. Deterrence/preventionExperimental and clinical
data suggest that renin-angiotensin system (RAS) antagonists and HMG-CoA
reductase inhibitors (statins) may decrease the incidence of AF and
increase the likelihood of successful cardioversion.
[42, 43, 44, 45] In
addition, treatment of underlying cardiovascular risk factors such as
hypertension, CAD, valvular heart disease, obesity, sleep apnea,
diabetes, and heart failure is likely to decrease the incidence of AF.
Fish oil preparations have also been shown to reduce ventricular
arrhythmias in at-risk populations (CAD) and may also protect against
AF.
Atrial Fibrillation MedicationFollow us