Hepatitis C Virus Infection Among Adolescents and Young Adults
Abstract and Introduction IntroductionHepatitis C virus (HCV) infection is a major cause of liver disease and hepatocellular carcinoma in the United States.
[1,2] Of the estimated 2.7–3.9 million persons with active HCV infection,
most were born during 1945–1964 and likely were infected during the
1970s and 1980s, before the advent of prevention measures.
[3] Nationwide, rates of acute, symptomatic HCV infection declined during 1992–2005 and then began to level.
[4] Declines also were observed in rates of newly reported HCV infection in
Massachusetts. Although these declines were evident among reported
cases overall in Massachusetts during 2002–2006, an increase was
observed among cases in the 15–24 year age group. In response to this
increase, the Massachusetts Department of Public Health (MDPH) launched a
surveillance initiative to collect more detailed information on cases
reported during 2007–2009 among this younger age group and to examine
the data for trends through 2009. This report describes results of both
efforts, which revealed continued increases in rates of newly reported
HCV infection among persons aged 15–24 years. These cases were reported
from all areas of the state, occurred predominantly among non-Hispanic
white persons, and were equally distributed among males and females. Of
cases with available risk data, injection drug use (IDU) was the most
common risk factor for HCV transmission. The increase in case reports
appears to represent an epidemic of HCV infection related to IDU among
new populations of adolescents and young adults in Massachusetts. The
findings indicate the need for enhanced surveillance of HCV infection
and intensified hepatitis C prevention efforts targeting adolescents and
young adults.
MDPH currently uses an electronic data system for disease
surveillance. All positive laboratory results indicating HCV infection
are reportable to MDPH. A positive laboratory result on a previously
unreported case prompts a case report form to be sent to the health-care
provider (e.g., clinician) ordering the test. This one-page form
collects information on demographics, symptoms, and risk history. In
accordance with CDC case definitions, HCV infection cases are classified
as either confirmed (i.e., positive by an anti-HCV antibody assay with a
nucleic acid test [NAT] result confirming active infection) or probable
(i.e., positive antibody test result with confirmatory NAT either not
conducted or not reported to MDPH). For this analysis, all confirmed and
probable cases of HCV infection were included.
In 2006, anecdotal information received from community-based partners
about HCV infection cases among adolescents and young adults prompted a
review of state surveillance data. Although an overall decline in rates
of newly reported HCV infection (from 181 to 128 cases per 100,000
population) was observed during 2002–2006, an increase (from 65 to 102
cases per 100,000 population) was observed among persons aged 15–24
years. At the time, 75% of 2005 surveillance reports for cases among
persons in this age group lacked risk history; therefore, the sources of
infection were unknown. Beginning in 2007, MDPH sent HCV infection case
report forms (CRFs) to reporting clinicians to collect additional
information when a report of newly identified HCV antibody (anti-HCV)
positivity among persons aged 15–24 years was received. Clinicians also
were sent reminders to fill out CRFs if more than 30 days had passed
from the date the form was sent and a completed form had not yet been
received by MDPH.
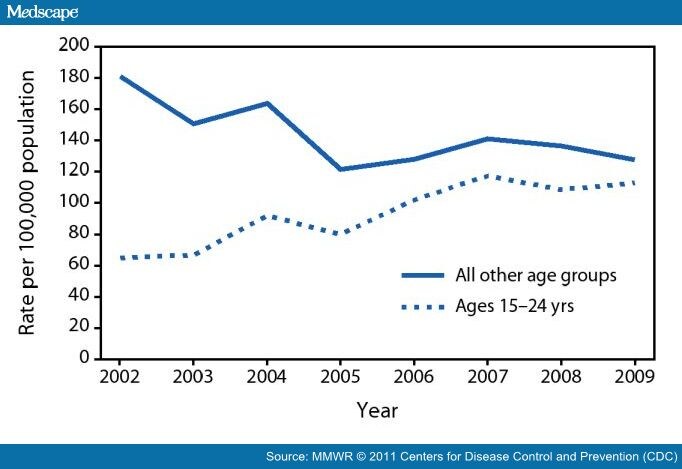
During 2002–2009, rates of newly reported HCV infection (confirmed
and probable) among persons aged 15–24 years increased from 65 to 113
cases per 100,000 population (Figure 1). The number of confirmed cases
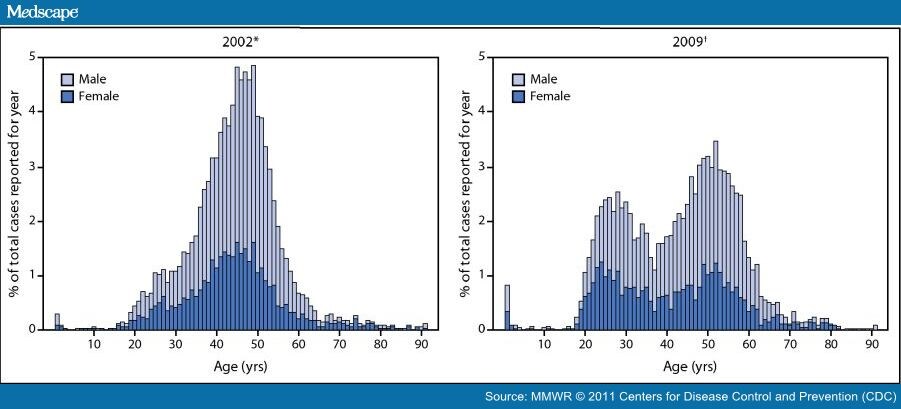
of HCV infection reported in Massachusetts was further examined by age
and compared for the years 2002 and 2009 (Figure 2). The data shifted
from a unimodal age distribution in 2002 to a bimodal age distribution
in 2009, with the latter showing substantially more reports of HCV
infection among adolescents and young adults compared with the earlier
period.
(Enlarge Image)
|
Figure 1.
Rates of newly reported cases
of hepatitis C virus infection (confirmed and probable) among persons
aged 15–24 years and among all other age groups — Massachusetts,
2002–2009
|
<blockquote>
</blockquote>
Figure 1. Rates of newly reported cases
of hepatitis C virus infection (confirmed and probable) among persons
aged 15–24 years and among all other age groups — Massachusetts,
2002–2009 
(Enlarge Image)
|
Figure 2.
Age distribution of newly reported confirmed cases of hepatitis C virus infection — Massachusetts, 2002 and 2009
* N = 6,281; excludes 35 cases with missing age or sex information.
† N = 3,904; excludes 346 cases with missing age or sex information.
|
<blockquote>
</blockquote>
Figure 2.
Age distribution of newly reported confirmed cases of hepatitis C virus infection — Massachusetts, 2002 and 2009 * N = 6,281; excludes 35 cases with missing age or sex information.
† N = 3,904; excludes 346 cases with missing age or sex information.
During 2007–2009, MDPH received 1,925 reports of new cases of HCV
infection among persons aged 15–24 years. Of these, 1,026 (53%) were
classified as confirmed cases of HCV infection; the remainder were
classified as probable. Although some clustering of cases was observed
in urban areas, cases were reported from all areas of the state,
including large metropolitan areas, suburban areas of Boston, smaller
cities, and rural areas. Cases occurred with nearly the same frequency
among men and women.
Of the 1,925 CRFs sent to reporting sources for completion, 1,448
(75%) were returned to MDPH, providing details of 802 confirmed and 646
probable cases. Of those returned, 252 (17%) CRFs did not have
sufficient information to assess risk, and of these, 148 (59%) contained
no risk data.
Of the total 1,448 CRFs returned, 1,357 (94%) included information on
race. Of these, 1,052 (78%) indicated cases among persons who were
white, 37 (3%) who were black, and 21 (2%) who were Asian; four
indicated cases among persons who were American Indian/Alaska Native,
and two indicated cases among persons who were Native Hawaiian or other
Pacific Islanders. Ninety-four CRFs indicated cases in persons reported
as being of unknown race, and 147 indicated "other" or multiple race
categories. Of 1,154 (80%) cases with ethnicity information, 98 (8%)
were among persons identified as Hispanic. Eight percent of the 1,448
cases with completed CRFs were among persons who were homeless or
incarcerated.
By far, the most common risk identified was IDU. Of 1,196 cases with a
reported risk history, 860 (72%) were in persons who reported current
or past IDU; of these, 719 (84%) reported injecting drugs during the
preceding 12 months. In addition, 445 (34%) reported some history of
intranasal drug use. All but 34 of the cases for which intranasal drug
use was listed also indicated IDU. Of the 719 cases for which IDU during
the preceding 12 months was reported, 615 (85%) were among persons who
reported heroin use, 220 (29%) cocaine use, seven (1%) methamphetamine
use, and 31 (4%) use of other drugs, including opiates other than heroin
(categories are not mutually exclusive because more than one drug could
be reported). Additional commonly reported potential exposures included
"other" blood exposures (24%) (further detail is missing for most cases
for which this was reported; for those cases with this information
included, a majority of "other" exposures listed were related to IDU),
tattoos (23%), and a history of incarceration (20%); however, most cases
involving these exposures were among persons who also were exposed
through IDU.
Editorial Note The Massachusetts surveillance data indicate an increase in HCV
infection cases among adolescents and young adults during 2002–2009.
These cases were primarily among non-Hispanic white residents in urban,
suburban, and rural communities. Although calculating an incidence rate
from the surveillance data or determining the duration of infection for
persons who tested positive for anti-HCV antibody is not possible, the
findings suggest that most persons aged 15–24 years with HCV infection
likely acquired their infections within a few years of being tested and
reported. Although similar increases in human immunodeficiency virus
(HIV) infection were not identified for this age group, increases in
reports of HCV infection among injection drug users might be a harbinger
of increases in IDU-associated HIV.
Other states have indicated similar increases in HCV infection among
adolescents and young adults. For example, in 2008, New York reported an
increase in HCV infection among persons aged <30 years in suburban
Buffalo.
[5] Since that time, surveillance data have indicated continued
transmission and possibly new activity in other areas of New York (Elena
Rizzo, New York State Department of Health, personal communication,
2011).
During the period when increases in HCV infection were being
observed, Massachusetts experienced a concomitant increase in heroin use
among adolescents and young adults. Data from MDPH-funded substance
abuse programs showed a rise in the percentage of admissions (for all
drug use) among persons aged 15–24 years, from 19% in 2002 to 23% in
2008.* Furthermore, the percentage of program clients who reported
needle use when admitted increased from 29% in 2002 to 38% in 2008 among
persons aged 15–24 years, whereas the percentage among all other age
groups during this same period remained relatively constant at
approximately 30%. Although the occurrence of IDU-associated HCV
infection has been documented for decades, the recent epidemic in
reported cases among adolescents and young adults and its apparent
association with increases in drug injection and sharing of injection
equipment in this population is a disturbing trend. Law enforcement data
suggest this trend might be occurring in other states. During
2002–2009, the estimated average annual number of heroin initiates in
the United States increased from 100,000 to 180,000.
† Law
enforcement reporting from the Great Lakes, Mid-Atlantic, New England,
New York/New Jersey, Southeast, and West Central regions also suggests
that heroin use is increasing, particularly among younger users.
§ Addressing the epidemic of HCV infection among adolescents and young
adults presents unique challenges in terms of education, outreach, and
other interventions. Studies have shown that the incidence of HCV
infection among injection drug users aged <30 years ranges from 10 to
37 cases per 100 person-years.
[6,7] Moreover, among adolescents and young adults who inject drugs, HCV
positivity has been associated with duration and frequency of injection.
[6] Adolescents and young adults might be more likely to share drug
equipment because of the nature of their social networks, which are
characterized by trust and sharing.
[6] The nature of these interactions must be taken into account when
developing educational materials. Adolescents and young adults are
likely to have participated in other risky behaviors before initiation
of injecting and might have multiple physical, mental, and emotional
health needs.
[8] The recent Institute of Medicine report on viral hepatitis and liver
cancer noted that younger injection drug users might be at highest risk
for seroconversion in the years immediately following initiation of
injection practices.
[2] The findings in this report are subject to at least four limitations.
First, the surveillance data only include information for persons who
have access to and obtain serologic testing and thus might
underrepresent the number of persons with HCV infection. This also might
explain, in part, the demographic patterns that were observed. Second,
efforts by MDPH to raise awareness of the increase in case rates among
this age group might have contributed to an increase in testing and
reporting of cases after 2007. Although data were not available to
ascertain whether this actually occurred, and if so, what the magnitude
of such an effect might have been, increases in the case rate among
adolescents and young adults in Massachusetts were evident in the years
before 2007 and, in fact, were more pronounced. In addition, recent
research on injection drug users showed that, although persons aged
18–24 years had the highest rate of being tested for HIV, they had the
lowest rate of HCV testing despite national recommendations for
counseling and screening of injection drug users.
[9,10] Third, differences by county of residence could not be determined
because of infrequent recording of residence information on laboratory
results not accompanied with a matching CRF. Finally, differences in
testing and reporting by county might also exist. Further studies are
needed to better characterize the population groups that are at
increased risk and those persons who are infected with HCV. Health-care
providers need to be encouraged to ask about risks for HCV infection,
especially IDU, and to screen patients at risk.
One important outcome of this study is that CDC, in collaboration
with state and local health departments, is examining HCV surveillance
data to determine whether similar trends are occurring in other
reporting areas. In addition, MDPH and CDC are conducting an in-depth
investigation of the causes of HCV transmission among adolescents and
young adults in Massachusetts to recommend and implement targeted
prevention measures.
This report highlights the important role of surveillance for HCV
infection and reporting of all laboratory tests positive for HCV, along
with the capacity to collect data of sufficient quality for meaningful
analysis of trends in transmission and disease. By 2010, 43 states
(including Massachusetts) and the District of Columbia required
reporting of all laboratory tests indicative of HCV infections.
¶ However, despite the laboratory reporting requirement, most states have
limited resources dedicated to surveillance of viral hepatitis and lack
capacity to investigate reported cases and forward reliable data to CDC
for national reporting. The Institute of Medicine noted this deficiency
in public health surveillance as a major weakness in the prevention of
viral hepatitis and liver cancer and recommended federal assistance for
states to effectively conduct surveillance for all forms of hepatitis C.
[2] This report also strongly indicates the need for expanded and
intensified hepatitis C prevention efforts targeting adolescents and
young adults. The Institute of Medicine notes that multicomponent,
comprehensive risk reduction programs are likely to be the most
successful at addressing HCV infection prevention needs of persons who
use illicit drugs. Some interventions that could be implemented include
access to sterile syringes and drug preparation equipment through
syringe exchange services, expanded school-based education that includes
viral hepatitis prevention messages, expanded harm reduction programs
directed toward young drug users, entry to drug treatment for young
injection drug users, and access to comprehensive health services that
include HCV testing and linkage to care.




